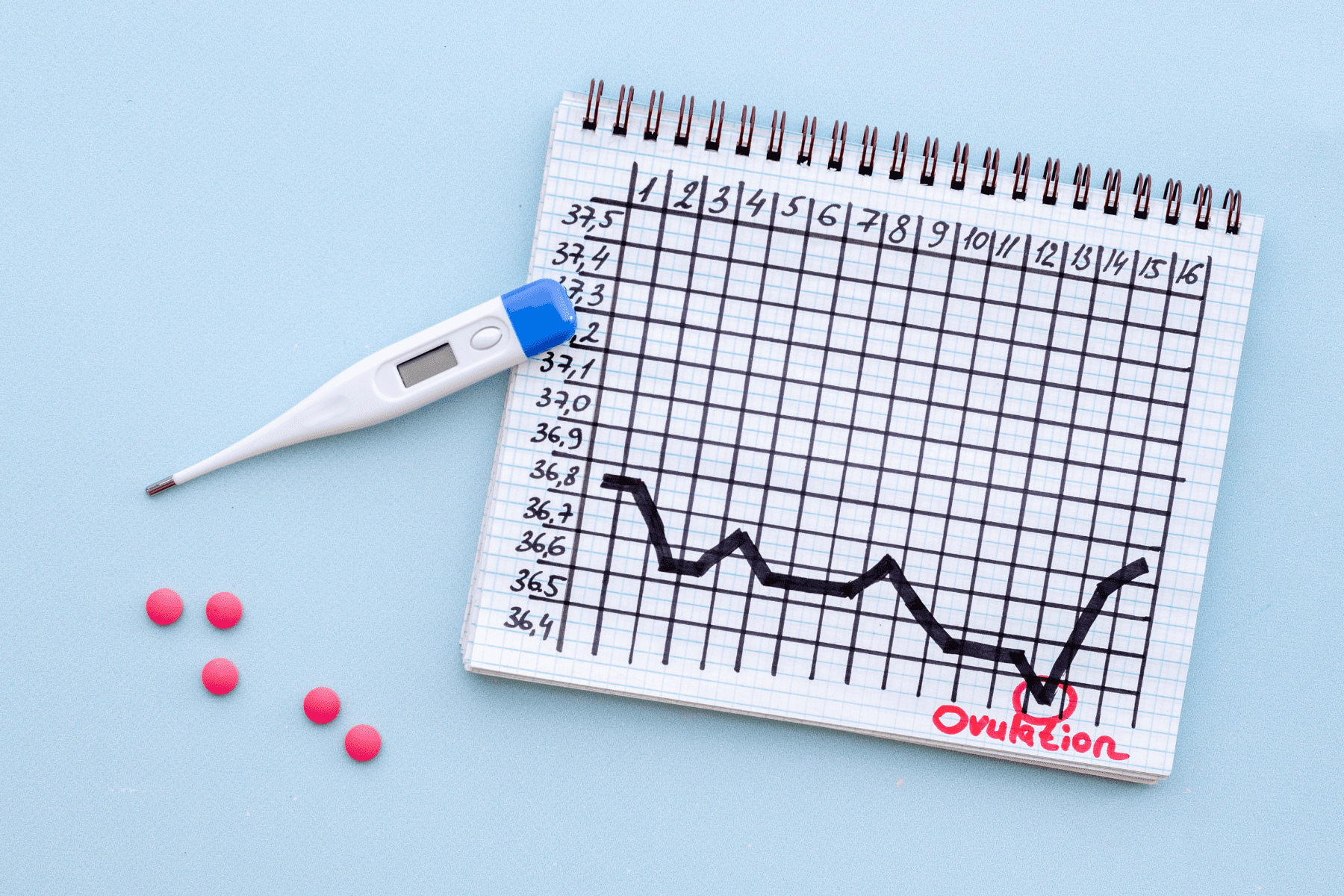
September is Polycystic Ovarian Syndrome (PCOS) Awareness Month, a disease and hormone disorder that affects one in 10 women of childbearing age in the U.S. PCOS is considered one of the top causes of infertility.
Fertility specialists have long been investigating the effects of PCOS on female fertility and how to best combat these challenges to help women achieve motherhood.
New research from Dr. Asima K. Ahmad of Fertility Centers of Illinois, completed during her time at the University of California, San Francisco, correlates advanced ovarian aging with a decline in a key female hormone.
In the study findings published by Fertility & Sterility, the research team monitored 31 women with PCOS against a control group of 266 and found that women with PCOS experienced faster rates of decline in antral follicle count (AFC) and anti-Müllerian hormone (AMH), both markers of ovarian reserve. When controlling for confounders, the decline in AFC was not statistically significant, but the faster decline continued with AMH.
What this means: women with PCOS may see their egg supply decline at a faster rate than women without PCOS.
To learn more about the study findings and their implications for women with PCOS, we discussed the study with Dr. Ahmad.
What is PCOS?
PCOS is a hormonal, or endocrine, disorder. Women can present with irregular menstrual cycles due to lack of or decreased frequency of ovulation, excess hair growth or acne and also have polycystic-appearing ovaries on ultrasound. One thing to keep in mind is that PCOS patients do not have “cysts” on their ovaries, but rather, we are looking for “follicles.” Follicles are fluid-filled sacs that surround growing eggs.
How is PCOS diagnosed?
PCOS can present in different ways, and can be diagnosed in more than one way. The Rotterdam Criteria evaluates three categories (ovulatory dysfunction, clinical signs of or elevated androgen (male hormone) levels, and polycystic-appearing ovaries):
1) Does the patient have irregular menstrual cycles?
2) Does she have clinical symptoms such as acne, excess facial or body hair, or hair loss (male-pattern hair loss)? Does she have excess levels of androgens?
3) Does she have polycystic-appearing ovaries?
If she meets two of these three criteria, and other etiologies have been ruled out, PCOS is present. This diagnosis is important, not only when it comes to fertility and reproductive health, but also overall health. Women with PCOS are at an increased risk of developing metabolic syndrome, diabetes, and cardiovascular disease in the future. Therefore, it is essential to discuss all aspects of this diagnosis with a patient such as uterine protection, management of hyperandrogenism, fertility potential and long term preventative health.
What do these findings mean for women with PCOS?
We already know that women with PCOS tend to have higher antral follicle count (AFC) and anti-Müllerian hormone (AMH) levels than those who do not. We also know that markers of ovarian reserve such as AFC, AMH and ovarian volume decrease with increasing age. However, this is one of the first large longitudinal studies of its size that analyzes the change and differences in ovarian reserve between these two populations. These findings are significant because they shed some light on the possibility that the rate of change in a woman’s ovarian reserve may be dependent on a pre-existing diagnosis such as PCOS. Having this information beforehand will assist with understanding fertility potential and making family planning choices.
How does anti-Müllerian hormone impact the reproductive process? What is optimal?
AMH is released by the cells surrounding a female’s eggs. Those with a relatively larger egg supply will have a higher AMH, therefore, having a higher AMH isn’t necessarily a bad thing. There is no optimal level for AMH, but an AMH of less than one can be considered diminished ovarian reserve. A woman’s AMH level declines with age as the egg supply decreases.
What is a common route of fertility treatment for women with PCOS?
Medications can be used to induce ovulation, such as clomiphene citrate or letrozole. Since PCOS patients have a higher follicle count, these medications should be given carefully and while monitoring a patient’s response to the medication through ultrasound or a blood test as they would be at high risk for multiple gestation. A study from the New England Journal of Medicine showed that the use of letrozole resulted in higher live birth and ovulation rates in women with PCOS as compared to clomiphene citrate. For those patients that are unresponsive to ovulation-inducing agents or who over-respond to these medications, the next step for treatment may be in-vitro fertilization.
What can women do to reduce the effects of PCOS on fertility?
Many lifestyle choices can reduce PCOS symptoms and encourage healthy cycles, which can help fertility. The basic tenets of healthy living also ring true for managing PCOS – opt for regular exercise, a healthy diet, and aim to be a healthy weight.
Sorry, no medical team available right now!