1. What is progesterone?
Progesterone, a naturally occurring hormone in the body, is produced by the corpus luteum, a hormone-secreting structure that develops from the follicle after an ovum (egg) has been released. It is also produced by the placenta during pregnancy. Each month, progesterone is released by the ovary and induces maturity of the uterine lining in preparation for pregnancy. When progesterone levels are abnormal, the individual may experience irregular menses, pregnancy loss, or infertility.
2. What role does progesterone play in fertility, conception and pregnancy?
Progesterone plays a major role in reproduction. Its synthesis by the ovary is initiated by ovulation. Sufficient amounts are needed to make the lining of the uterus ready for implantation of the embryo and maintenance of pregnancy. If this production is inadequate, supplementation may be necessary. Prior to eight weeks of gestation, the production of progesterone is mainly derived from the corpus luteum located in the ovary. It is critical that progesterone levels support pregnancy during these early stages to prevent pregnancy loss. After that timeframe, progesterone is mainly derived from the placenta of the growing fetus.
3. What infertility issues does progesterone help to address?
Progesterone supplements are commonly used in women with infertility diagnoses such as ovulatory disorders, recurrent pregnancy loss, and in conjunction with Assisted Reproductive Technology (In Vitro Fertilization, Embryo Transfer, Frozen Embryo Transfer, etc.) Progesterone supplements help to compensate for low production of the hormone after ovulation.
4. How do you determine if someone needs progesterone?
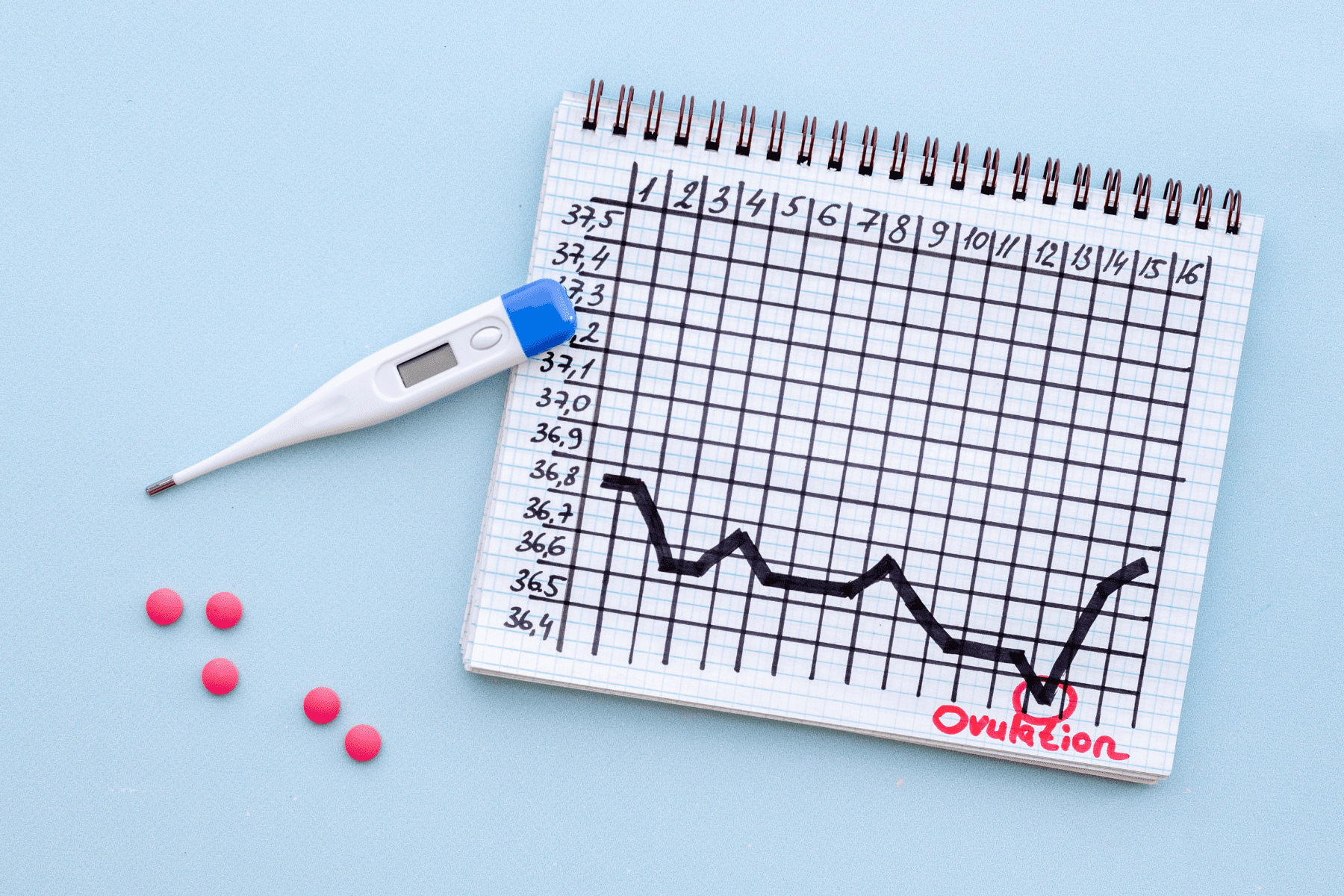
First, a patient’s medical history is assessed. Having abnormally short cycles or early recurrent pregnancy loss may be due to inadequate progesterone production. Blood tests to measure progesterone levels a week after ovulation may be attempted in women with regular menses but this does not have much clinical significance. A biopsy of the uterine lining may even be done (although an uncommon practice these days) to determine a lack of progesterone effect. Sometimes, progesterone is used empirically, that is, just to make sure enough progesterone is delivered to the uterine lining.
5. How is progesterone incorporated in an IVF cycle?
During the egg retrieval process, the cells that normally create progesterone after ovulation are removed along with the eggs. Progesterone supplements are then required to prepare the body for pregnancy and mature the uterine lining to support successful embryo attachment in the womb. Continuation of progesterone supplementation is advisable, on an individual basis, even up to 10 weeks of pregnancy in a cycle where embryo transfer is done.
6. What are the side effects of progesterone?
Depending on the route of administration, there may be no side effects, especially with vaginal preparations, which have a direct uterine effect, rather than a systemic one. Vaginal discharge or irritation are possible with these forms. If injectable or oral preparations are used, side effects may include pain, swelling and bruising at the injection site, headaches, breast tenderness, drowsiness, dizziness, fluid retention, bloating, hot flashes, constipation, and everything that mimics pregnancy symptoms! These symptoms may persist into a pregnancy as well, or stop when the drug is withdrawn.
7. Is progesterone safe for my baby and me?
Natural progesterone, which is used during fertility treatment, poses no threat to a mother and child. It is important to note that the Food and Drug Administration (FDA) does not differentiate between natural progesterone and synthetic progesterone (progestins) in its warnings. Progestins are mostly used to suppress ovulation and are found in birth control pills. They are only used in preparation for fertility treatment. In older studies synthetic progestins have been linked to a slightly increased risk of certain birth defects if used during pregnancy. The FDA has conducted a thorough review of relevant published studies and has found there is no increase in birth defects resulting from exposure to any progesterone in early pregnancy.
8. What different types of progesterone are prescribed?
During fertility treatment, a woman may be prescribed the following progesterone supplements in these common doses:
- Crinone 8% (vaginal gel, once or twice per day)
- Endometrin (vaginal tablets, 100mg 2-3x/day)
- Progesterone in oil (intramuscular injection, 50-100 mg once a day)
These three routes noted above have been shown to be effective in fertility treatment. Less reliable are:
- Prometrium (oral tablets, also prescribed for vaginal use, 200 mg 1-2x/day)
- Progesterone suppositories (200 mg 1-2x/day, compounded by a pharmacy. Not FDA approved and unregulated)
The decision of what progesterone supplement will be used is dependent upon a physician’s judgment and personal preferences, as well as a patient’s particular situation.
In the past, intramuscular injections were commonly used as a result of the lack of other available preparations. Multiple studies have shown that in certain types of treatment cycles, there is no difference in the outcome when compared to vaginal progesterone. An additional advantage of vaginal progesterone is that it does not cause the pain of intramuscular progesterone injections. In some circumstances, combinations of different types of progesterone may be prescribed.
9. What costs are associated with progesterone medication?
Compared to other fertility drugs, progesterone tends to be less expensive, and insurance generally covers one form or another.
10. Who is not a candidate for progesterone medication?
Patients who have had an allergic reaction to one form of progesterone should be switched to another form, even in the middle of treatment. Allergy is typically towards the substance that progesterone is compounded with (type of oil for example) and not to the hormone itself. Side effects specific to a certain form of progesterone administration are also a reason to switch.
Medical contribution by Elie Hobeika, M.D.
Dr. Hobeika is board certified in both Obstetrics and Gynecology and Reproductive Endocrinology and Infertility. He has studied with world leaders in PCOS and recurrent pregnancy loss and is fluent in English, French, and Arabic.